
Never mind Reefer Madness, seniors are the next big cannabis consumers
on December 3, 2019
It’s a quiet Monday afternoon at Magnolia Oakland, a cannabis dispensary on the industrial end of Adeline Street.
From the outside, the blocky, concrete building looks like the kind of place you might go to get a package shipped or a document notarized. Inside, as a guy working security chats with a front desk employee checking IDs, a skunky whiff of weed floats by, indicating that this is, in fact, a place to legally buy a bewildering number of cannabis products. The glass cases inside are stocked with dozens of varieties of corpulent, furry cannabis flower packed in zipped packages or rolled up into joints; tins of CBD mints and candy weed gummies; and bottles and jars of tinctures and topical rubs. At Magnolia, you can even consume or vape onsite. This is a marijuana mecca.
It’s particularly quiet today, especially for a Monday, when seniors get 20 percent off. More and more older Americans are using cannabis to soothe a litany of aches and ailments that accompany a long life. Insomnia, chronic pain, and anxiety are just a few common afflictions that seniors are turning to cannabis for. A 2019 study published in Drugs and Aging from researchers at the University of Colorado concluded that cannabis use by adults over age 65 is increasing more quickly than among all other age groups. The study also found that between 2006 and 2013, the rate of past-year marijuana use among those over 50 increased by 71.4 percent.
Even still, some older adults still feel a stigma against using cannabis. The same study surveyed 136 people over 60, some of whom said they were reluctant to discuss cannabis use even with their doctor. Many preferred to pay more to buy it recreationally, instead of receiving a medical card from a provider.
Here in Oakland, when seniors and other first-timers walk into Magnolia, they are likely to be welcomed by Barbara Blaser, the dispensary’s 74-year-old registered nurse on duty. Blaser, who is known around the shop as “Nurse Barbara,” has an open face, and wears rhinestone jeweled glasses, red fringed earrings and speaks with a slight Midwestern clip.
“I think that I provide a non-stigmatizing face,” she said. “I think of myself as a cannabis guide, [helping] you through this massive amount of information.” She is quick to note that she cannot suggest any products—it is illegal for nurses to prescribe or recommend medication. That’s what the budtenders behind Magnolia’s shiplap wooden bar are here for, politely waiting to guide customers through the wide world of legal weed retail.
Nurse Barbara, instead, practices what she calls “reality therapy.” A patient can set up an hour-long appointment with her, and she’ll explain her own cannabis journey: from denial, to acceptance, to evangelism. “I’ve seen it change people’s lives,” she said.
Blaser’s been a nurse for a half-century, first in the Department of Psychiatry at the University of Chicago. After she and her husband moved to California 15 years ago to be with their kids, she took a job working as a hospice and long-term care nurse. At that point, she had never tried cannabis, even though her daughter is Debby Goldsberry, a well-known cannabis advocate who’s been active since the 1980s. In 1999, Goldsberry founded the Berkeley Patients Group (BPG), a medical cannabis collective and the country’s longest-running dispensary. The BPG staff has been advocating for access to medical cannabis since its inception, and was involved in the fight for state legalization. Today, Goldsberry is the executive director of Magnolia.
Blaser says years before, when people asked what she thought about her daughter’s work, she would always reply, “It’s not my issue. It’s not my job.” But a debilitating illness five years ago left Blaser in a comatose state, relying on a ventilator and a feeding tube. As she recovered, she was left with chronic pain and insomnia. Her daughter begged her to try cannabis, but she spent a couple of months doing research, first. “The more I learned, the more interested I became,” she said. And once she tried it, it worked.
Now, Blaser is becoming the reason many customers come to Magnolia in the first place. She was written about in the San Francisco Chronicle. “Last month I was in the AARP bulletin,” she said.

Some seniors come for help with insomnia, some for anxiety, and some for lack of appetite. Some have been sent by doctors who suggest that they try marijuana to treat chronic pain. “Some people will say, ‘I just want to be able to garden. I want to be able to laugh again,’” Blaser said. She teaches a series of classes at Magnolia: “Cannabis 101 for Seniors,” “Microdosing Magic,” “Improving your Sexual Experience with Cannabis.”
And she said many people have had an experience similar to her own. “It was interesting the number of people who were my age, whose children had said, ‘You’ve suffered long enough, just try this,’” she said. “And when they would come here, sometimes against their will, and they would see me—a regular old lady, fully-functional—then they were willing to try.”
If a person comes into Magnolia saying they haven’t slept in years, Blaser will put together a packet with the latest research on cannabis and insomnia, and hand out an anxiety checklist with suggestions of what to do before bed to relax. She’ll go over the person’s evening routine, and talk about what their goal is. She will ask about their current medications and previous medical issues and evaluate how these might be affected by using cannabis.
In her consultations, she’ll explains the differences between tinctures and edibles, and how pain can be managed depending on the method of ingestion. “Tincture goes under your tongue … and works in 7 to 10 minutes, but only lasts two hours,” she said. “An edible takes two hours to work but lasts 5, 7, 8 hours.”
She never suggests a specific product or dose, instead more generally advising clients to “start low and go slow,” to write down the dosage, and not to do it alone. “You tell someone that you’re going to try cannabis, or you ask someone to be home with you. Because sometimes people don’t tell anybody,” she said. “Well, that’s not very safe.”
*****
It’s a weeknight at the downtown Oakland public library and Dr. Laurie Vollen, a slight woman wearing a boxy blazer, turtleneck and a silk scarf, is deftly explaining the difference between cannabidiol (CBD) and Tetrahydrocannabinol (THC), the two primary active compounds in the cannabis plant. (THC is the main psychoactive component and is also the one responsible for getting you stoned.) Vollen is presenting a PowerPoint in a dim basement room to a small crowd of silver-haired women and one middle-aged man who smells faintly of marijuana.
A general practitioner who specializes in the medical application and prescription of cannabis, Vollen teaches these free public lectures called “Cannabis and Aging” in libraries around the Bay Area each month.
Her interest in cannabis was sparked several years ago when some of her patients told her that they were substituting cannabis for anti-anxiety, anti-depressant, and insomnia medications like Halcydol, Prozac, and Klonopin. “And they were finding that not only was [cannabis] satisfactory in terms of effectiveness, but it had no side effects,” said Vollen in a later interview in her office. “And after doing what little research could be done at that time, I basically could not find any literature suggesting that medicinal doses of cannabis had any ill effects. Whereas you can’t say the same for all the other pharmaceutical medications they were taking.”
But the more she researched, the more she realized there wasn’t much information in the medical community to help patients find the right dose of medicinal cannabis to use. “So that’s when I opened up my own office that is really focusing on giving the comprehensive facilitation necessary for the effective adoption of this medicament,” she said.
Since recreational marijuana use became legal in California in 2016, Vollen has seen the patient roster for her private practice grow older, with patients looking for relief from ailments like back and shoulder pain, insomnia, arthritis, Parkinson’s disease, multiple sclerosis, anxiety, and depression. And most don’t want to get stoned.
“The most oft-spoken words in my office are, ‘I don’t want to get high,’” she said, adding that you don’t need to feel high for the dose to be effective. In fact, she considers feeling high a side effect of taking too much. “Everyone has a sweet spot where they get the medicinal benefits without the adverse side effects and they do not get high,” she said. “And what that is for each individual is largely determined by genetics.”
In her talk at the Oakland library, she cautioned her audience about finding the right dose. “Of all the things that cannabis has impressed me [about], the game-changer, as a physician, is anxiety. CBD is a game changer for anxiety,” she said. But she was careful to note that taking too high a dose can cause anxiety.
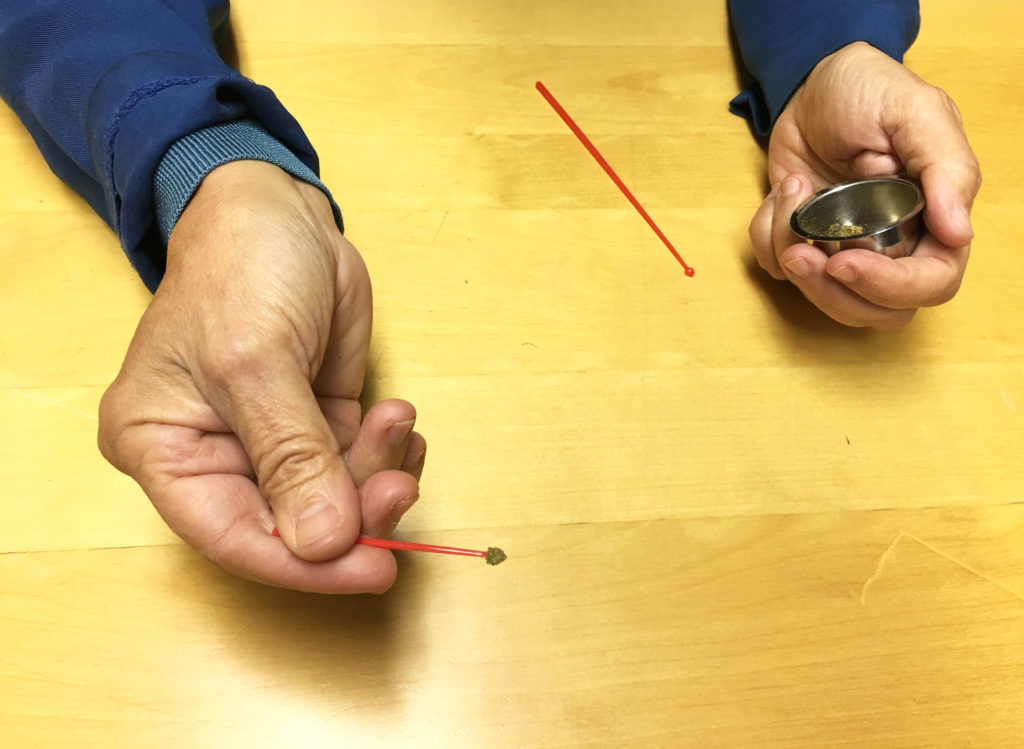
As she clicked through her presentation, she told her audience about a 2010 double blind, placebo-controlled study on pain relief performed by Mark Ware from McGill University Health Centre, and published in the Canadian Medical Association Journal, which concluded that inhaling a low dose of THC three times a day can alleviate chronic pain and improve sleep.
She flipped her next slide, showing a very tiny ball of weed, which was the equivalent of the dose used in Ware’s study: 2.5 mg of THC in a strain of cannabis that is 25 percent THC. “It’s hard for you to see, but it is about a quarter of the size of my little fingernail bed,” she said. “And for most patients, [this dose] is effective and cost-efficient. Depending upon where you buy your bud, if you can buy a gram for $13, one dose will cost you 13 cents.”
She says that most dispensary staffers don’t know how to guide patients to such small medicinal doses, because it’s not a cost benefit to their business model. So Vollen leads a popular class called “Inhalation 101,” teaching a particular method for smoking such a small amount of weed. “I teach patients how to smoke medicinal amounts of cannabis, because there is no way that you’re going to figure out how to do this on your own,” she said.
And because cannabis is a plant, bred in hundreds of varieties with varying percentages of THC and CBD, and sold in many different forms, it’s not as easy to regulate dosing as it is for, say, pharmaceutical pills. So Vollen works with patients to record their dosage and increase the amount slowly and deliberately until they find that sweet spot.
As she concludes her library presentation, the audience members have questions: One woman asks about inflammation. One is a caretaker for her husband and wants to know how cannabis would interact with his medications. The stoned man says he wants to get down to a dose that is medically effective, and quit getting stoned everyday. After she answers their questions and they file out the door, nearly everyone picks up a brochure about Vollen’s private practice and cannabis classes.
*****
Though openly using marijuana is becoming more common, especially on the West Coast, Vollen and Blaser say that some seniors are still reluctant to try it because of its stigma. Part of that has to do with the drug’s long history of being federally restricted.
Medical marijuana was first legalized in California in 1996, with the passage of Proposition 215. In 2016, the state’s legalization of recreational use followed through Proposition 64. Though it’s medically legal in 33 states, federally, marijuana is still illegal and considered a Schedule 1 drug by the Drug Enforcement Administration (DEA). This category is used for drugs that are determined to have no medical value and to be susceptible to abuse.
Some advocates are calling for cannabis to be rescheduled, saying that research shows that the drug has medical benefits. It has long been studied in Israel and Canada. But as long as cannabis remains a Schedule 1 drug in the United States, it’s difficult for US researchers to obtain permission for the large scale clinical trials that are necessary to determine whether a drug is safe and effective according to standards set by the Food and Drug Administration (FDA).
If passed, the Marijuana Opportunity Reinvestment and Expungement (MORE) Act might change that. Written by presidential candidate Senator Kamala Harris, the law would effectively end the federal prohibition of cannabis in the United States, removing it from Schedule 1. (It also proposes a broad set of criminal justice reforms, including expunging the criminal records of previous cannabis offenders.) It passed the House Judiciary Committee on November 20, but still needs to be considered by the entire House of Representatives. If it passes there, it would head to the US Senate.
Even if the bill doesn’t pass, policies permitting randomized clinical trials are slowly changing at the state level. The Colorado Public Health Department has funded such a study which will assess for the first time how cannabis compares to Oxycodone for chronic pain relief. The study is being conducted by the University of Colorado, Denver and will be completed by 2020.

For seniors, this current federal prohibition is significant in other ways, too. Because of marijuana’s Schedule 1 classification, nursing homes and assisted living facilities could lose their federal funding if they are caught dispensing it, said Beth Hoddess, who practices tax, elder and cannabis law for OnPoint Legal Council, PC. She’s also the president of the board of directors of a non-profit skilled nursing facility, Chaparral House in Berkeley.
“A facility cannot have their nurses administering cannabis, because then they’ve inserted themselves into essentially breaking federal law,” said Hoddess. She says there are workarounds—some facilities will allow patients to self-administer or allow a family member to supply the drug. “But it really creates a dilemma in terms of regulations regarding administering medication and who does it,” she said.
Hoddess said that cannabis can relieve anxiety and increase appetite, and she believes that the quality of life of nursing home residents would increase dramatically if they could rely on medical cannabis, reducing a reliance on prescription medications that can cause negative side effects. For example, she said that drugs like Haldol and Seroquel, antipsychotic drugs that are used in hospital settings to treat confusion and improve concentration, are administered too often to older patients in skilled nursing facilities. She said that workers at understaffed facilities sometimes overmedicate patients in order to sedate them, so the staff won’t need to attend to each patient as often. These drugs can be used to “reduce labor costs, if you can make residents reduce their needs by essentially medicating them,” she said.
But these drugs can have severe side effects. Haldol can cause mental changes, renal failure and risk of death when given to elderly patients with dementia, and the fine print attached to Seroquel also warns of changes of mood or behavior, and a slight increase in the risk of death when administered to the elderly.
In the 2019 University of Colorado study on senior cannabis use, the researchers also found that despite the legalization of cannabis there and other states, some older people still felt a stigma. “Some participants, for example, referred to the movie Reefer Madness and other anti-marijuana propaganda adverts that negatively framed cannabis as immoral and illegal,” the study’s authors noted. Reefer Madness, a propaganda film from 1936, depicts disasters befalling unsuspecting teenagers who smoke marijuana. The film was originally produced by a church group as a cautionary tale, and later re-cut in the 1940s for the exploitation film circuit. It’s since become a cult classic, now seen for its campy and outrageous claims and underlying racism. But it did have an effect on the way a lot of people of that generation thought about cannabis.
Melodye Montgomery is the founder of the T’Oakland Senior Cannabis Club, a social club whose members meet once a month to socialize and use cannabis in a judgement-free setting. “A lot of seniors aren’t able to talk to their families about their cannabis use because we’re still dealing with that stigma, with that Reefer Madness,” she said.
Montgomery says she’s been smoking weed since she was 17, and that throughout her life it has helped her social anxiety. Now age 60, she takes capsules, uses topical creams and smokes flower to help her cope with arthritis and chronic pain in her hips, shoulders and elbows, the legacy of a 20-year-career as a professional artistic roller skater. (“Same thing that you see on ice skating, we did on roller skates,” she said.)
“Typically, if you’re not using cannabis at this stage as an ex-athlete, you’re heavy on pain-relieving drugs,” she said.
In fact, a 2016 study published in The Journal of Pain by researchers at the University of Michigan, Ann Arbor found that among the 374 participants, medical cannabis use was associated with a 64 percent decrease in opioid painkiller use, and an improved quality of life.
*****
Peter Sussman, a 78-year-old former editor of The San Francisco Chronicle, is a former weed smoker who has come back to cannabis as he’s gotten older. He says he smoked pot recreationally when he was in his 20s, but ditched his stash when Berkeley police officers took an interest in his political activity. (The activity in question was his attempt to hire a helicopter to hover over a city council meeting in protest of the police department petitioning for a helicopter of its own to patrol protests.)
The helicopter he rented never showed, but the police did. They contacted the Chronicle and he got called into the editor’s office over the stunt, Sussman said. (For the record, Sussman said, his editors told the police that what employees do in their free time is their own business.)
“When I became aware that they were aware of my activities, I thought it was not a good idea to have a stash,” he said with a laugh. Sussman said he never gave it up entirely, smoking occasionally at parties, but didn’t keep it in the house any longer.
A few years ago, he began experiencing very painful jabs in his shoulder from which he couldn’t find relief. Eventually, he got a medical cannabis card and began experimenting with tinctures. A nephew who worked at a dispensary helped him navigate through different strains with varying levels of THC and CBD, and after much experimentation he found the right ratio.
“It didn’t help me that much with the pain, maybe took the edge off it a little bit, but it was wonderful for sleep,” he said. He’s since had several surgeries on his shoulder, but continues to use cannabis for his insomnia. Sussman said he used to frequent a neighborhood dispensary but now relies on the “concierge service” of a local cannabis dispensary that delivers. “It comes right to the door and you don’t have to worry about it,” he said.
But for some, the fellowship at Magnolia is a draw, along with the fact that customers can consume their cannabis on site. At the dispensary on senior discount day, a 60-year-old named Margo, who declined to give her last name, was at the dab table. Dabbing is a way to inhale cannabis—instead of smoking or vaping the flower, here a waxy cannabis concentrate is heated through an electric dab rig, which looks like a high-design electric bong. Consumers can buy a small tub of concentrate at Magnolia and sit around the table, passing the rig and taking puffs as if it were a hooka. For Margo, though, it’s a solitary ritual.
“It’s like a coffee shop for me,” said Margo, who found her way to dabbing after being treated for Stage 4 esophageal cancer that had moved to her liver. She said that she was in enormous pain from the cancer treatments, which included having her stomach removed and eating through a feeding tube. “So you’re on morphine, you’re on codeine, you’re on Percocet. And you’re drinking it because you can’t swallow a pill,” she said. She was miserable and nauseous, and a nurse friend recommended that she try cannabis for relief. “And so I started slowly. Someone got me a volcano,” she said, referring to an early model smokeless cannabis vaporizer. “And finally I felt good. It was like a miracle. [Magnolia] is the first place I ever came.”
She said that as part of the “Reefer Madness generation” she hid her use for a while, adding that she thinks cannabis still has a stigma for a lot of people her age. But for her, with time and regular use, the stigma has faded. She’s been coming to Magnolia every Monday since to take a turn at the dab table. “It’s so gentle, it overtakes you. I know a lot of people my age say they don’t want to get high, but I definitely want that THC,” she said. She went back to the dab, and took another deep breath in.


Oakland North welcomes comments from our readers, but we ask users to keep all discussion civil and on-topic. Comments post automatically without review from our staff, but we reserve the right to delete material that is libelous, a personal attack, or spam. We request that commenters consistently use the same login name. Comments from the same user posted under multiple aliases may be deleted. Oakland North assumes no liability for comments posted to the site and no endorsement is implied; commenters are solely responsible for their own content.

Oakland North
Oakland North is an online news service produced by students at the UC Berkeley Graduate School of Journalism and covering Oakland, California. Our goals are to improve local coverage, innovate with digital media, and listen to you–about the issues that concern you and the reporting you’d like to see in your community. Please send news tips to: oaklandnorthstaff@gmail.com.


